Anal and Peri-Anal Warts
Anal warts are one of the most common sexually transmitted infections in world. They are caused by a small DNA virus, a papillomavirus belonging to the papovavirus group, which cannot be cultured. Genital warts differ from skin warts histologically and antigenically. Genital warts are nearly always
transmitted by sexual contact; autoinoculation from hand to genitals is unusual. The infectivity of sexually acquired warts is about 60%; the incubation period is long, varying from two weeks to eight months.
Four distinct sub-types of Ano-genital warts have been described: condylomata acuminata (pointed warts), flat / macular lesions, papular, and keratotic lesions. The first two sub-types are mainly found on moist, non-keratinized epithelia, while the latter two usually present on keratinized epidermis. Ano-genital warts are also often referred to as genital warts, condylomata acuminata or genital verruca.
Anal/ peri-anal/ Ano-genital warts are highly infectious; approximately 65% of individuals with an infected partner develop the lesions within 3 weeks and 8 months after exposure, the median time between infection with HPV types 6 or 11 and the development of warts was 11 to 12 months among males and 5 to 6 months among young females. In rare cases, Ano-genital warts can be associated with malignant lesions, namely Buschke-Lowenstein tumors.
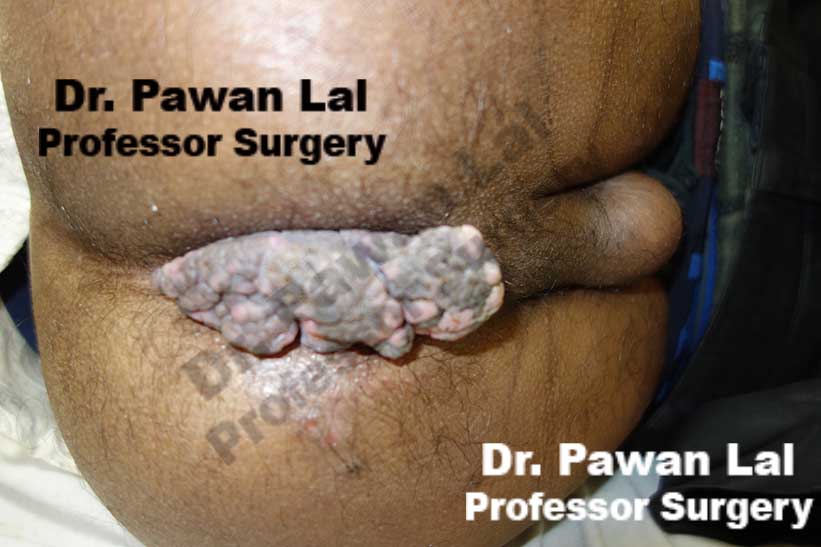
 Multiple Peri-anal warts (Condyloma acuminata)
Multiple Peri-anal warts (Condyloma acuminata)

Multiple Peri-anal warts (Condyloma acuminata)
Diagrammatic representation of Anal Warts is shown below
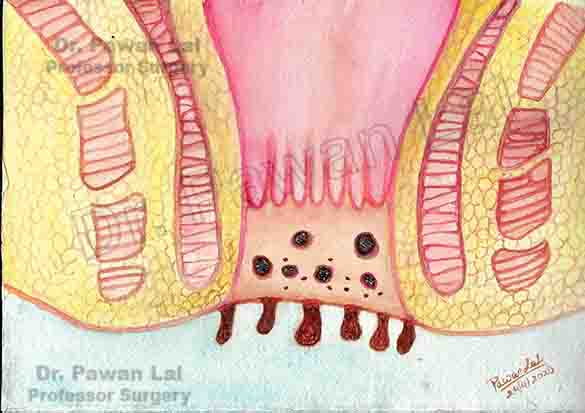
Diagram showing warts in the Anal canal and peri-anal skin (Also Anal verge)
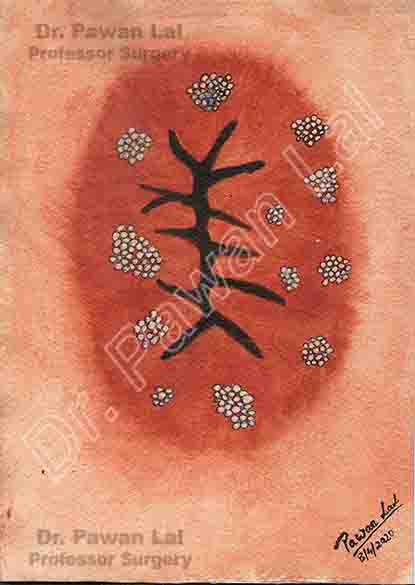
Peri-anal and Anal Warts (Diagramatic)
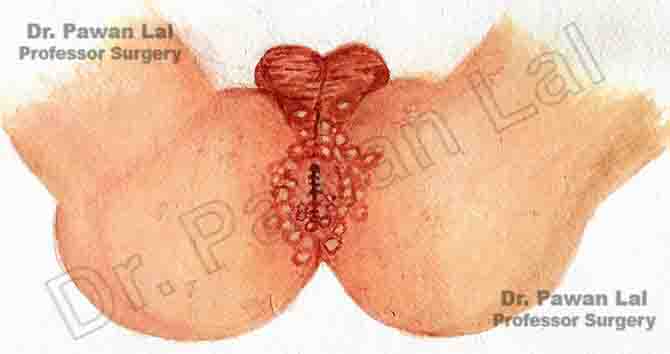
Peri-anal and Anal Warts (Diagramatic)
Symptoms of Anal Warts
Anal warts are a commonly transmitted sexual infection among young adults. It is a painless condition and most are unaware as there are no symptoms. There is a common complain of anal itching. Tiny spots or growths can be seen and also can be felt with fingers. When they become large, one may feel a lump or mass in the anal area. The other symptoms noticed in anal or peri-anal warts are bleeding or increased mucus discharge. pain, itching, burning, irritation,
The infection with Human papilloma virus (HPV) can cause emotional and psychological problems with the person which includes shame, embarrassment, anger, depression and guilt. Since the Anal and Peri-anal warts are caused by ano-receptive sex, they are either not reported early either due to non-visualization or due to shame/guilt. The lesions can be handled easily when they are reported early. Presence of peri-anal lesions can cause cessation of sexual activity of patients, either through fear of transmission or embarrassment of lesions.
Cutaneous (skin) HPV types
Most HPV types are called cutaneous because they cause warts on the skin, such as on the arms, chest, hands, and feet. These are common warts, not genital warts.
Mucosal (Genital or Anogenital) HPV types
The other HPV types are considered mucosal types because they invade and live in cells on mucosal surfaces. The mucosal HPV types are also called genital (or anogenital) HPV types because they often affect the anal and genital area. These types can also infect the lining of the mouth and throat. Mucosal HPV types generally don’t grow in the skin or parts of the body other than the mucosal surfaces but can involve anal and perianal skin surface as shown in the picture below. Mucosal (genital) HPV is spread mainly by direct skin-to-skin contact during vaginal, oral, or anal sexual activity. It’s not spread through blood or body fluids. It can be spread even when an infected person has no visible signs or symptoms.

Click for large image
Low-risk mucosal (genital) HPV types: HPV types that tend to cause warts and rarely cause cancer are called low-risk types. Low-risk genital HPV infection can cause cauliflower-shaped warts on or around the genitals and anus of both men and women. In women, warts may appear in areas that aren’t always noticed, such as the cervix and vagina.
High-risk mucosal (genital) HPV types: HPV types that can cause cancer are called high-risk types. These types have been linked to certain cancers in both men and women. Doctors worry about the cell changes and pre-cancers these types cause because they are more likely to grow into cancers over time6.
Anyone who has had sexual contact can get HPV, even if it was only with only one person, but infections are more likely in people who have had many sex partners.
The virus can also be spread by genital contact without sex, but this is not common. Oral-genital and hand-genital spread of some genital HPV types have been reported. And there may be other ways to become infected with HPV that aren’t yet clear.
You DO NOT get HPV from:
- Toilet seats
- Hugging or holding hands
- Swimming in pools or hot tubs
- Sharing food or utensils
- Being unclean
Transmission from mother to newborn during birth is rare, but it can happen, too. When it does, it can cause warts (papillomas) in the infant’s breathing tubes (trachea and bronchi) and lungs, which is called respiratory papillomatosis. These papillomas can also grow in the voice box, which is called laryngeal papillomatosis. Both of these infections can cause life-long problems.
Patients should be reassured that if they have developed anal/ peri-anal / Ano-genital warts, appropriate treatment can clear the warts within 3 months. The anal/peri-anal lesions are of mostly sexual origin and are caused by Human Papilloma Virus (HPV) which is contagious; therefore, it is important for patients to disclose their recent sexual partners, who should be advised examination to rule out Human papilloma virus (HPV) infection. The smokers have a 27% increased risk of developing anal/peri-anal (ano-genital) warts as compared with non‐smokers. The HPV prevalence in patients who smoke is 48.2% compared with 37.5% for non‐smokers (P < 0.001). Generally, warts develop within weeks or months after acquiring Human Papilloma Virus (HPV) infection but in a significant number of cases, the virus can be dormant for months or years before warts emerge.
HPV Screening Through Anal Cytology
Though there is no guidelines for anal screening for HPV or anal cytology for anal cancer lesion (precancerous or abnormal anal canal cytology) but there is benefit if getting the anal Cytology for Anal cancer screening (similar to cervical cancer screening), using anal cytology (through canal brush cytology) followed by referral of patients with abnormal results to high-resolution anoscopy and subsequent treatment of biopsy-proved AIN (Anal canal Cancer in situ), may prevent the development of anal cancer.
The reported sensitivity and specificity of anal cytology relative to findings at biopsy (sensitivity, 69%-93%; specificity, 32%-59%, respectively) are similar to findings in studies comparing cervical cytology and cervical biopsy for the prevention of cervical cancer. There is definitive benefit to do annual anal cytology for MSM (men having sex with men) and any HIV-positive patients with a history of anogenital condylomas. Among patients with HIV- or HPV-related lesions, histologic signs of dysplasia are apparent in more than one-fifth of those who undergo testing. Among HIV-positive MSM (men having sex with men), the positive predictive value of abnormal anal cytology to predict anal dysplasia is approximately 95%.
Anal cytology can distinguish between the various stages of Anal Intra-epithelial neoplasia (AIN) 9.
- Low-grade dysplastic cellular changes (AIN 1).
- severe dysplasia (AIN 2)
- Severe dysplasia and cancerous changes but no invasion (AIN 3), also known as carcinoma in situ, is diagnosed when 50% of the epithelial tissue is replaced with abnormal dysplastic cells.
Buschke–Lowenstein Tumor - Buschke–Lowenstein tumor, often called giant condyloma accuminatum, is considered by some authors as intermediate between condyloma and squamous cell carcinoma. Histologically, the tumor appears benign with papillomatosis, epithelial hyperplasia, and koilocytosis, but clinically it can behave aggressively with extensive infiltration. Typically, it is slow growing in immunocompetent individuals, but it can grow rapidly in immunocompromised individuals. Focally, these tumors can transform into invasive carcinoma; hence, early diagnosis and treatment is crucial. Common treatment approach includes radical surgical resection with tumor-free resection margins. Prophylactic HPV vaccination has been shown to reduce HPV6/11 infection and anogenital condylomata and thus is expected to prevent this tumor12, 13, 14.
Technique of anal Cytology for collecting the specimen
The goal of anal cytology is to identify patients with cellular changes in the epithelial cells that line the anal canal; any patients with atypia are then referred to undergo high-resolution anoscopy. No specific preparation is necessary before anal cytology, though patients should be instructed to refrain from receptive anal sex and enemas for 24 hours before testing. If a digital rectal examination is performed in conjunction with anal cytology, the cytologic sample must be obtained before lubrication is introduced into the anal canal. The standard technique used in obtaining anal cytologic specimens involves inserting a water-moistened Dacron swab into the anal canal to above the squamocolumnar transition zone, approximately 2 cm (1 inch) from the anal verge. While mild external pressure is applied to the anal wall, the swab is gently manipulated in a craniocaudal and circular motion within the canal. After several rotations, the swab should be withdrawn and immediately immersed in methanol-based preservative-transport solution.
High Resolution Anoscopy by high powered microscope (Anoscope / colposcope) for screening for intra-epithelial tumors of anal canal
The patient is put in jack knife position to expose anal canal. The anal canal is opened by inserting a Anal retractor (Czerny rectal speculum)

The anal canal is then screened segment by segment. The anal skin is treated with acetic acid 3% to see any aceto-white lesions and then treated with Lugol's iodine. Any area that does not take up the iodine is suspcious area and biopsy is taken from that area.
Treatment of Anal Warts
Treatment options include patient-applied (home-based) chemical treatments (podofilox, imiquimod), physician applied (office-based) chemical treatments (podophyllin, trichloracetic acid, interferon, green tea extract) and ablative treatments (cryotherapy, surgical removal, laser treatment). The main limitation of current therapies is the high recurrence rate after initial remission. The quadrivalent HPV vaccine demonstrated high efficacy in preventing the onset of HPV 6/11-related Ano-genital Warts in both males and females.
Treatment should be individualized for each patient. Although untreated warts can resolve spontaneously, most patients want an immediate intervention to eradicate them. Treatments need to be selected on the basis of considerations such as the number, size, morphology, location and keratinization of warts, and whether they are new or recurrent.
Ablative techniques
Ablative techniques are commonly used to remove warts. The major frustration is the high rate of recurrence with these treatments and the need for repeat therapeutic interventions. Ablative techniques are associated with a risk of bleeding, tissue destruction, slow wound healing and scarring
| Treatment | Mode of action | Schedule | Clearance rate (%) | Recurrence rate (%) | Advantages | Disadvantages |
| Ablative Techniques | ||||||
| Electrocautery | High‐frequency electrical currents cause thermal damage to infected tissue | Under local anaesthesia, base of lesion excised; repeat as required |
90% (Range:35–94%) |
20% (Range:20-25%) |
90% |
High recurrence rate is used alone but with immunomodulator creams the results are more than 90% remission rate Repeat physician visits Expertise required Smoke evacuator needed |
| CO2 and Nd:YAG laser | Laser vaporizes lesions | Under local anaesthesia, protocol depends on type of laser |
90% (Range:23–95%) |
70% (Range:2.5–77%) |
Rapid results Effective for thick lesions |
High recurrence rate; in some cases even before healing of laser treatment Costly Substantial training & Expertise required Pain/scarring Smoke evacuator needed |