Fistula in Ano or an anal fistula is an abnormal connection between the anal canal and the skin.
FISTULA IN ANO or ANAL FISTULA or PERI-ANAL FISTULA

Anatomy
The anal canal is the terminal (end) portion of the gastrointestinal tract. Two concentric rings of muscle, the internal anal sphincter and external anal sphincter, surround the anal canal. The internal anal sphincter is composed of smooth muscle and is not under voluntary control. The external anal sphincter is composed of skeletal muscle and is under voluntary control. Together these two muscles are very important in the maintenance of continence.
Approximately one to two centimeters inside the anal canal, the lining of the anal canal changes. There is a line that marks this change called the dentate line. Anal glands located between the concentric layers of the internal and external anal sphincters empty into the anal canal at the level of the dentate line.
Causes and Symptoms
Nearly all anal fistulae are a result of an anorectal abscess. An anorectal abscess begins with infection in one of the anal glands. The infection may stay in the space between the sphincters (the intersphincteric space), may spread down to the perianal skin, or may extend through the external anal sphincter.
With an anorectal abscess usually pain and a tender swelling around the anus is present. Treatment is usually straightforward and consists of incising the skin over the abscess in order to drain the contained pus. Treatment following drainage of the abscess usually consists of sitz baths several times a day and use of bulk forming agents. Antibiotics are rarely necessary. Over the next several weeks the abscess wound gradually heals.
A fistula-in-ano results when there is failure of the abscess wound to heal completely. Most people with a fistula-in-ano give a history of having an anorectal abscess that was either drained surgically or spontaneously drained. About 50% of patients with an acute anorectal abscess go on to develop a chronic fistula-in-ano. The primary symptom of a fistula-in-ano is persistent drainage due to chronic, low grade sepsis (infection) after treatment of the acute abscess.
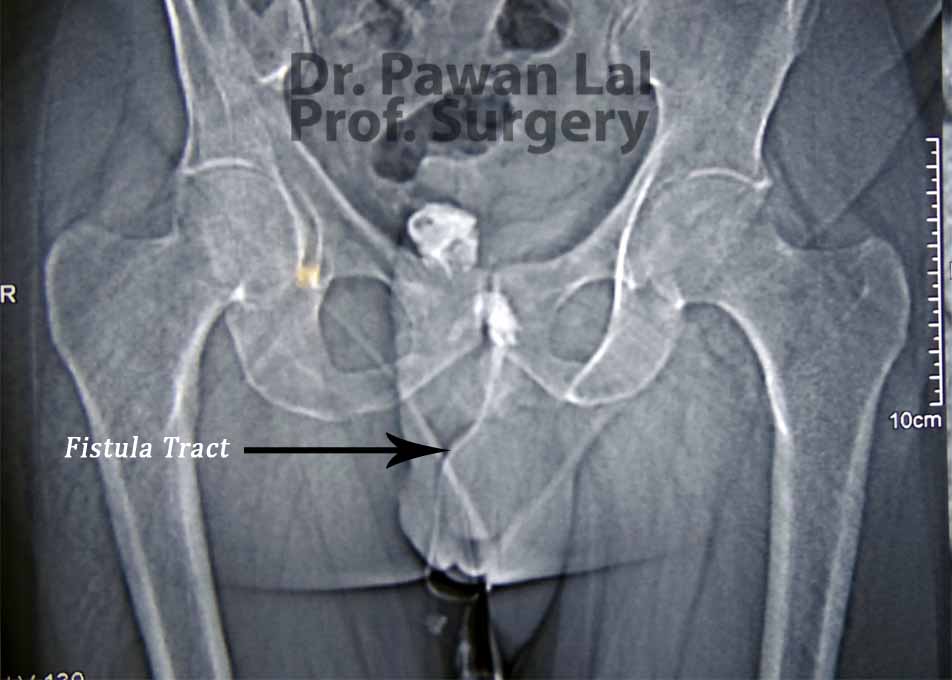
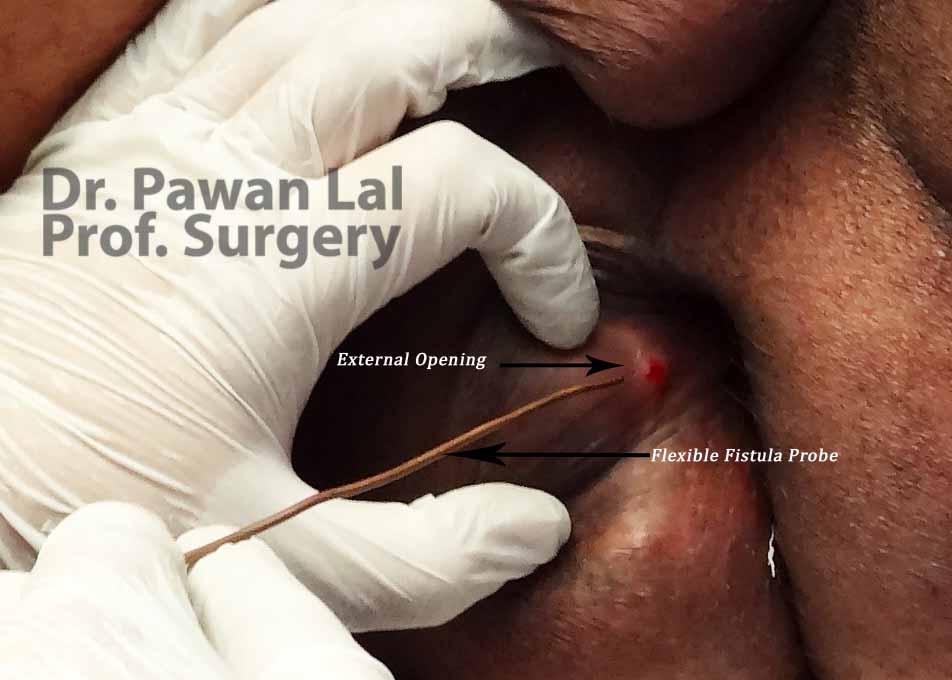
Diagnosis of a fistula-in-ano rests on identifying the external opening on the perianal skin and the internal opening in the anal canal.
Investigations
Treatment
The goals of treatment of a fistula-in-ano are the elimination of sepsis and of the fistula tract, the prevention of recurrence, and the preservation of continence. A fistula-in-ano always traverses or passes through a portion of the internal anal sphincter and usually some, if not all, of the external anal sphincter.
Treatment of an anal fistula requires surgery in an operating room under general or regional anesthesia. The majority of fistulae can be managed by simply laying open the fistula tract. This involves dividing the overlying tissue, which includes a portion of the sphincter complex. The chronic inflammatory tissue is removed and the wound is allowed to heal secondarily by scar tissue formation.
For fistulas that involve the internal anal sphincter or only a small portion of the external anal sphincter there is a small risk of incontinence postoperatively. The greater the amount of external sphincter traversed by the fistula, the greater the risk of postoperative incontinence after the lay-open technique.
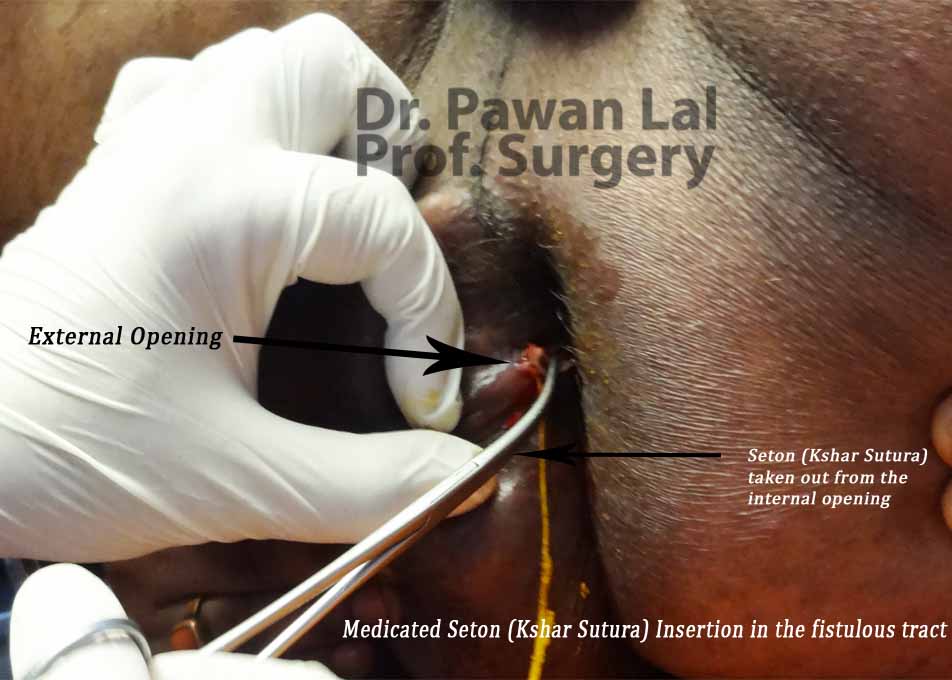
Alternative treatments are available for persons in whom the risk of incontinence would be too great using this technique. The most commonly used method is the use of a seton.
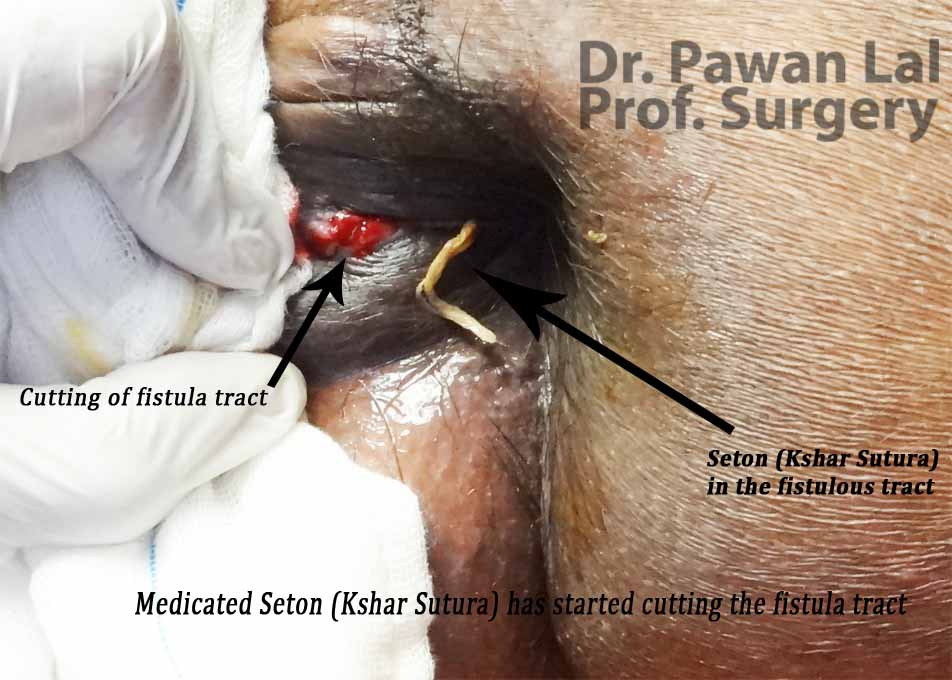
A seton is a thread passed around the fistula tract. It can be made of many different materials including silk or nylon suture, rubber, or plastic. Setons can be used in many different ways. They can act as drains to prevent recurrent infections. They can mark the site of a fistula tract to permit it to be divided in stages, thus reducing the chance of postoperative incontinence. Finally, they can be intermittently tightened to slowly cut through the sphincter muscles. The rationale here is that healing and scarring occurs as the seton cuts through the muscle, preventing division of the muscle all at once.
For a patient with a fistula that is not amenable to either the lay-open technique or treatment with a seton, there are a number of more complex surgical procedures available live VAAFT, fibrin glue, Fibrin plug or by creation of a flap of tissue in the anal canal to cover the internal opening in combination with drainage of the external opening and fistula tract.
Summary
Fistulas recur in less than 10% of patients after surgery. Fistula-in-ano is a common condition that usually follows infection of an anal gland. Treatment is directed at eliminating infection, while preventing recurrence and incontinence after surgery.
Most patients are readily treated by simply laying open the fistula tract. Other available options include the use of setons, VAAFT, Fibrin glue, fibrin plug or advancement flaps.
References
1. Sherief Shawki, Steven D Wexner. Idiopathic fistula-in-anoWorld J Gastroenterol 2011 July 28; 17(28): 3277-3285